Effective: 04/06/2023
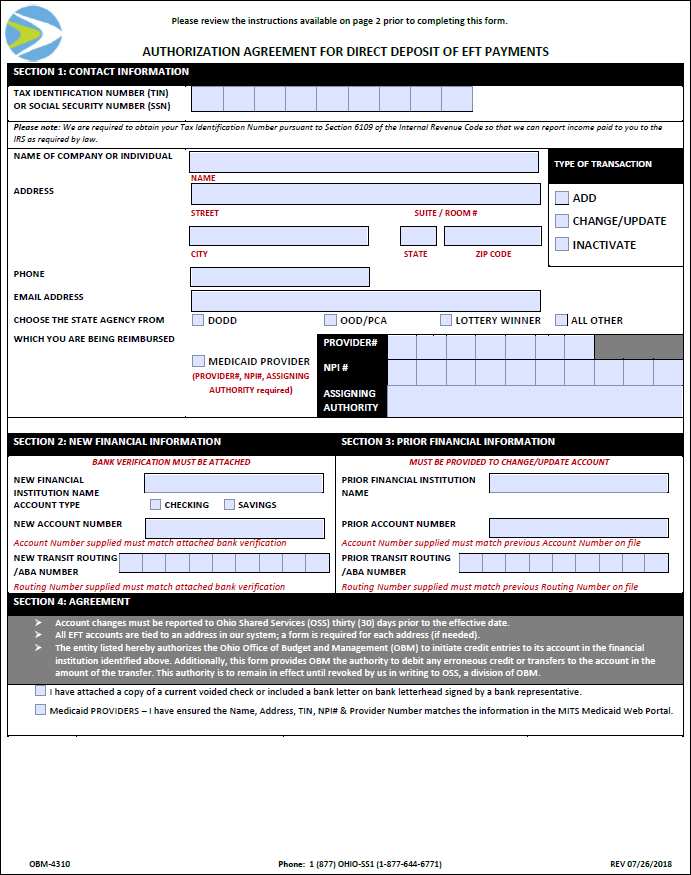
The preferred method of payment for the State of Ohio is EFT (Electronic Funds Transfer). The "Authorization Agreement for Direct Deposit of EFT Payments" (OBM-4310) is used to enroll in the EFT program and/or submit changes to the EFT information on the supplier record (see Entering or Changing Supplier EFT Information). Supplier Operations forms are available through the State of Ohio Suppliers website.
Bank Verification must be provided for:
A document from the financial institution or screenshot from an online-only bank/prepaid card is acceptable if it meets these requirements:
When a municipality (e.g., "Ashland County) is trying to setup direct deposit for a particular division (e.g., "Health Dept"), the department name must be listed on the "Authorization Agreement for Direct Deposit of EFT Payments." The "Authorization Agreement for Direct Deposit of EFT Payments" must be signed by the Treasurer / Fiscal Officer / Finance Manager / Trustee when sharing the Treasurer's depository account or it must be accompanied with a letter signed by the Treasurer stating that the division shares the account.
If a division is listed for a municipality and it's accompanied by a Treasurer's check, a letter from the Treasurer (or Auditor) stating that the division shares that account, must be attached or the Treasurer must sign the EFT form. The imprinted address for the Treasurer does not have to match.
If the municipality does not have a Treasurer's check, it may be substituted with a check from the Auditor with bank verification.
EFT forms and bank verification with varying naming conventions for Government Entities and divisions including acronyms/abbreviations, such as Clerk / Trustee / Treasurer / Fiscal Officer / Finance Manager, along with other terms that reference a municipality (e.g., County, District, Township, Village, or Corporation) are acceptable.
Can also be signed by Judge/Deputy Clerk.
For municipalities, the address on bank verification is not required for process.
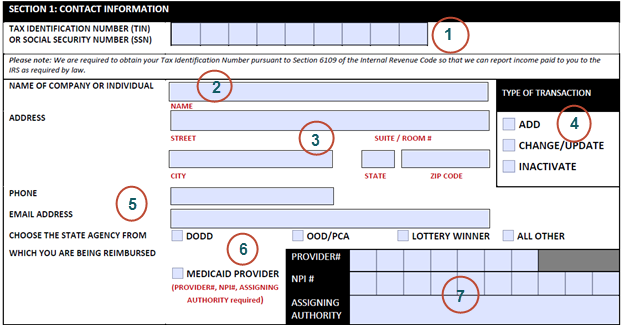
Tax Identification Number or Social Security Number must be completed. (Must have 9 digits and match the VIF, W9, OAKS- Supplier module on the Identifying Information tab or Maintain EFT module on the Maintain EFT tab, and/or MITS - where applicable).
Name of Company or Individual must be completed. (Must match the VIF, W9, OAKS- Supplier module on the Identifying Information Tab or Maintain EFT module on the Maintain EFT Tab, and/or MITS - where applicable).
If the supplier is listed with a formal name and bank verification comes with a shortened name (e.g., William / Will), the forms will be accepted.
Click here for MedicaidMedicaid.
A stamped name and address is acceptable (excluding the signature line).
Address – a complete address must be provided. (Must match VIF, OAKS- Supplier module on the AddressAddress tab, MITS, and/or bank verification - where applicable).
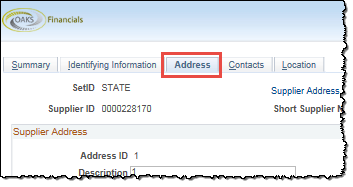
All EFT accounts are tied to a specific address in the Supplier Operations module and either a form is required for each address or multiple addresses may be listed in Section 1 (if needed).
If the "Authorization Agreement for Direct Deposit of EFT Payments" form provides multiple addresses, setup will be determined by the type of bank verification attached:
Voided Check - only addresses on the voided check are entered.
Bank Communication - all addresses on the form are entered.
Prepaid Card - only addresses on the prepaid card verification are entered.
Type of Transaction
Phone & Email Address are not required; however, if provided will be used for notification purposes.
Choose the state agency from which is being reimbursed - If this section is not completed, the type of action and the documentation needed will be determined when reviewing MITS, the OAKS FIN Supplier Module, or Maintain EFT module.
If "Medicaid Provider" is checked, the appropriate information must be listed in the Provider, NPI, Assigning Authority section.
Provider, NPI, Assigning Authority - When the 7-digit Medicaid Provider Number is listed on the form, it must match the provider number and name listed in MITS and/or OAKS-Maintain EFT module. NPI and Assigning Authority are required by the Federal Government; however, they are not needed for OSS processing.
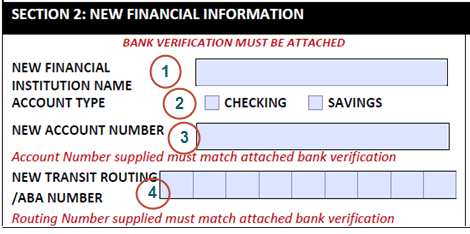
New Financial Institution Name is not required.
Account Type is not required since it can be determined by the banking verification provided or by contacting the bank.
If the type of account is not on the Bank Verification, but it is on the "Authorization Agreement for Direct Deposit of EFT Payments" form (or vice versa), the form(s) can be processed.
If the type of account is conflicting between the "Authorization Agreement for Direct Deposit of EFT Payments" form and the bank verification, contact the bank for confirmation.
If the type of account is not listed on the "Authorization Agreement for Direct Deposit of EFT Payments" form, but a voided check is included, the form(s) can be processed.
Money Market accounts are entered as checking accounts unless otherwise noted.
New Account Number must be completed and must match the bank verification.
Acceptable to process if zeros are omitted from the beginning of the account number or the check number is included at the end of the account number on the EFT form.
New Transit Routing/ABA Number must be provided on either the form or the bank verification.
Verify the bank routing number when it is missing from either the form or bank verification via the Routing Number website or by contacting the bank.
Verify the bank routing number when it does not match between the form or bank verification via the Routing Number website or by contacting the bank.
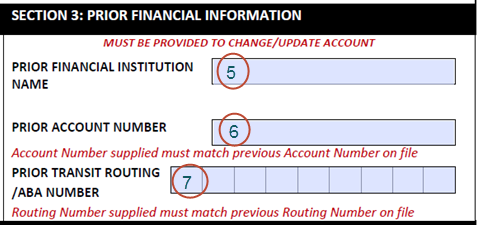
If a supplier / provider is unable to retrieve their old bank account information, they may obtain a letter from their prior bank stating that their old bank account information cannot be located.
Verify the bank routing number when it does not match between the form or OAKS FIN via the Routing Number website or by contacting the bank.
If the bank routing numbers belong to the same financial institution, the form can be processed.
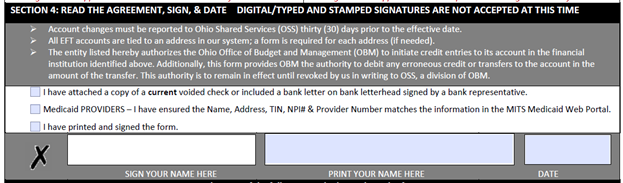
Read, Sign, and Date must be handwritten.